Hammer Toe Modification Surgery
 Overview
Overview
Hammer toe, also called hammer toe, deformity of the second, third, or fourth toe in which the toe is bent downward at the middle joint (the proximal interphalangeal [PIP] joint), such that the overall shape of the toe resembles a hammer. Most cases of hammertoe involve the second toe, and often only one or two toes are affected. In rare cases when all the toes are involved, a thorough neurological assessment is necessary to evaluate for underlying nerve or spinal cord problems.
Causes
Most hammertoes are caused by wearing ill-fitting, tight or high-heeled shoes over a long period of time. Shoes that don?t fit well can crowd the toes, putting pressure on the middle toes and causing them to curl downward. Other causes include genes. Some people are born with hammertoe, bunions. These knobby bumps sometimes develop at the side of the big toe. This can make the big toe bend toward the other toes. The big toe can then overlap and crowd the smaller toes. Arthritis in a toe joint can lead to hammertoe.
 Symptoms
Symptoms
Symptoms of a hammertoe are usually first noticed as a corn on the top of the toe or at the tip which produces pain with walking or wearing tight shoes. Most people feel a corn is due to a skin hammertoe problem on their toes, which in fact, it is protecting the underlying bone deformity. A corn on the toe is sometimes referred to as a heloma dura or heloma durum, meaning hard corn. This is most common at the level of the affected joint due to continuous friction of the deformity against your shoes.
Diagnosis
Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred.
Non Surgical Treatment
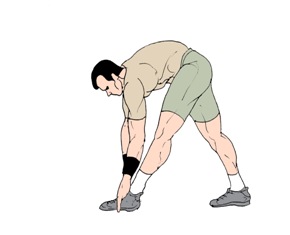
If the affected toe is still flexible, you may be able to treat it by taping or splinting the toe to hold it straight. Your family doctor can show you how to do this. You may also try corrective footwear, corn pads and other devices to reduce pain. You may need to do certain exercises to keep your toe joints flexible. For example, you may need to move and stretch your toe gently with your hands. You can also exercise by picking things up with your toes. Small or soft objects, such as marbles or towels, work best. If your hammer toe becomes painful, you may need to apply an ice pack several times a day. This can help relieve the soreness and swelling. Nonsteroidal anti-inflammatory medicines (also called NSAIDs), such as ibuprofen (two brand names: Advil, Motrin) or naproxen (one brand name: Aleve), may be helpful. If your pain and swelling are severe, your doctor may need to give you a steroid injection in the toe joint.
Surgical Treatment
If these non-invasive treatments don?t work, or if the joint is rigid, a doctor?s only recourse may be to perform surgery. During the surgery, the doctor makes an incision and cuts the tendon to release it or moves the tendon away from or around the joint. Sometimes part of the joint needs to be removed or the joint needs to be fused. Each surgery is different in terms of what is needed to treat the hammertoe. Normally after any foot surgery, patients use a surgical shoe for four to six weeks, but often the recovery from hammertoe surgery is more rapid than that. An unfortunate reality is that hammertoe can actually return even after surgery if a patient continues to make choices that will aggravate the situation. Though doctors usually explain pretty clearly what needs to be done to avoid this.
What Are The Principal Reasons For Over-Pronation
Overview
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.

Causes
For those not familiar with the term pronation, you might be familiar with terms related to shoes and pronation such as ?motion control?, ?stability,? and ?neutral cushioned.? The terms motion control and stability are typically associated with the word ?over-pronation? or a foot that is supposedly pronating too much and needs correction. According to the running shoe industry, ?over-pronation? is a biomechanical affliction evident when the foot and or ankle rolls inward past the vertical line created by your leg when standing.
Symptoms
Because pronation is a twisting of the foot, all of the muscles and tendons which run from the leg and ankle into the foot will be twisted. In over-pronation, resulting laxity of the soft tissue structures of the foot and loosened joints cause the bones of the feet shift. When this occurs, the muscles which attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. Injuries due to poor biomechanics and twisting of these muscles due to over-pronation include: shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). Foot problems due to over-pronation include: bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammer toes, and calluses.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.

Non Surgical Treatment
Although there is no actual cure for over-pronation it is possible to correct or at least reduce this problem. In order to restore our normal foot function an 'orthotic' or orthotic insole device is placed inside the shoes. Orthotics are designed to realign the foot and ankle bones to their natural position. This in turn restores our normal foot function and it helps alleviate not only foot problems but also ailments in other parts of the body i.e. the legs, knees and lower back. In addition to wearing an orthotic, it is recommended to wear supportive shoes, like good quality athletic footwear with a firm heel counter and sufficient flexibility in the forefoot area.
Surgical Treatment
The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain.
Heel Ache The Causes, Indications And Therapy Options
Overview

Does it feel like you have a nail in your heel? After walking for a few minutes does the pain slowly disappear? Millions of people each year are faced with this type of Heel Pain. While there may be other causes, the most common is Plantar Fasciitis. Plantar Faciitis is an inflammation of the fibrous tissue, called the plantar fasciia, that runs along the bottom of your foot that connects the heel (calcaneus) to the toes (metatarsals). Treatment for this condition can take many forms including: stretching exercises, drugs, orthotics, injections, and in rare cases surgical procedures. Until now the treatment methods have addressed the active conscious periods only to be undone when a person goes to bed or sits in the easy chair relaxing.
Causes
Heel pain has a number of causes that are typically associated with overuse of the heel bone. You can strain your heel by pounding your feet on hard surfaces, being overweight, or wearing shoes that do not fit properly. These strains can irritate the heel?s bones, muscles, or tendons. Other common causes of heel pain include the following. Heel Spurs. Heel spurs develop when the lining that covers the heel is continuously stretched. When this occurs, pieces of the lining may break off. Heel spurs typically develop in athletes who frequently run or jog. They are also common in people who are obese. Plantar Fasciitis. Plantar fasciitis develops when the tissue connecting the heel to the ball of the foot becomes inflamed. Plantar fasciitis also occurs in athletes who frequently run or jog. It can also result from wearing shoes that do not fit properly. Excessive Pronation. Excessive pronation occurs when the ligaments and tendons at the back of the heel are stretched too much. This condition can occur when injuries to the back, hips, or knees change the way you walk. Achilles Tendinitis. Achilles tendinitis can occur when the Achilles tendon, which runs along the back of the heel, becomes inflamed. This condition is common in people with active lifestyles who frequently run and jog, professional athletes and dancers.
Symptoms
Symptoms may also include swelling that is quite tender to the touch. Standing, walking and constrictive shoe wear typically aggravate symptoms. Many patients with this problem are middle-aged and may be slightly overweight. Another group of patients who suffer from this condition are young, active runners.
Diagnosis
A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem.
Non Surgical Treatment
Treatment of heel pain depends on its cause. Plantar fasciitis. Most doctors recommend a six- to eight-week program of conservative treatment, including temporary rest from sports that trigger the foot problem, stretching exercises, ice massage to the sole of the foot, footwear modifications, taping of the sole of the injured foot, and acetaminophen (Tylenol) or nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin or ibuprofen (Advil, Motrin and others) for pain. If this conservative treatment doesn't help, your doctor may recommend that you wear a night splint or a short leg cast, or he or she may inject corticosteroid medication into the painful area. Surgery is rarely necessary and is not always successful. Heel spur. Conservative treatment includes the use of shoe supports (either a heel raise or a donut-shaped heel cushion) and a limited number of local corticosteroid injections (usually up to three per year). As in plantar fasciitis, surgery is a last resort. Calcaneal apophysitis. This condition usually goes away on its own. In the meantime, conservative treatment includes rest and the use of heel pads and heel cushions. Bursitis. Treatment is similar to the treatment of heel spurs. Changing the type of footwear may be essential.
Surgical Treatment
Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
Prevention

A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don?t underestimate your body's need for rest and good nutrition. If obese, lose weight.
What Could We Do About Achilles Tendinitis Suffering ?
Overview
 Achilles tendinitis describes an inflammatory change of the Achilles tendon without a tear of the tendon. Achilles tendinitis may be acute or chronic. The onset of pain is usually unilateral but may be found bilaterally. Achilles tendinitis is common in the third or fourth decade of life in patients who are active with sports or in jobs that require physical labor. Pain is described at the insertion of the tendon in the heel bone or in the body of the tendon.
Achilles tendinitis describes an inflammatory change of the Achilles tendon without a tear of the tendon. Achilles tendinitis may be acute or chronic. The onset of pain is usually unilateral but may be found bilaterally. Achilles tendinitis is common in the third or fourth decade of life in patients who are active with sports or in jobs that require physical labor. Pain is described at the insertion of the tendon in the heel bone or in the body of the tendon.
Causes
Tendinitis typically develops after abrupt changes in activity or training level, use of poorly fit or worn footwear, or training on uneven or dense running surfaces. Overuse prior to sufficient training is generally the cause. This is due to forces 8-10 times the body weight acting on the tendon during physical activity. Achilles injuries range from inflammation to a breakdown in the tendon. Pain is generally felt low on the back of the heel due to the low vascularity and susceptibility for inflammation. Pain higher on the Achilles is generally more muscular pain and less tendonitis. If swollen spots or knots are found along the tendon, or if the tendon feels jagged, cease activity and seek professional medical care.
Symptoms
Symptoms vary because you can injure various areas of the muscle-tendon complex. The pain may be an acute or chronic sharp, stabbing, piercing, shooting, burning or aching. It is often most noticeable immediately after getting out of bed in the morning, or after periods of inactivity, like sitting down for lunch. After a couple minutes of walking around, it will often then settle down somewhat, before becoming symptomatic again after excessive time standing or walking. But regardless of how the pain is perceived, Achilles tendon pain should not be left untreated due to the danger that the tendon can become weak, frayed, thickened, and eventually it may rupture.
Diagnosis
A doctor or professional therapist will confirm a diagnosis, identify and correct possible causes, apply treatment and prescribe eccentric rehabilitation exercises. An MRI or Ultrasound scan can determine the extent of the injury and indicate a precise diagnosis. Gait analysis along with a physical assessment will identify any possible biomechanical factors such as over pronation which may have contributed to the achilles tendonitis and training methods will be considered. Biomechanical problems can be corrected with the use of orthotic inserts and selection of correct footwear.
Nonsurgical Treatment
The aim of the treatment is to reduce strain on the tendon and reduce inflammation. Strain may be reduced by, avoiding or severely limiting activities that may aggravate the condition, such as running, using shoe inserts (orthoses) to take pressure off the tendon as it heals. In cases of flat or hyperpronated feet, your doctor or podiatrist may recommend long-term use of orthoses. I8nflammation may be reduced by, applying icepacks for 20 minutes per hour during the acute stage, taking non-steroidal anti-inflammatory drugs, placing the foot in a cast or restrictive ankle-boot to minimise movement and give the tendon time to heal. This may be recommended in severe cases and used for about eight weeks. Occasionally depot (slowly absorbed) steroid injections may be tried, particularly for peri-tendinitis, but great care needs to be taken to avoid injecting into the tendon. This should only be done by a specialist doctor. You may also be given specific exercises to gently stretch the calf muscles once the acute stage of inflammation has settled down. Your doctor or physiotherapist will recommend these exercises when you are on the road to recovery. Recovery is often slow and will depend on the severity of the condition and how carefully you follow the treatment and care instructions you are given.

Surgical Treatment
Surgery can be done to remove hardened fibrous tissue and repair any small tendon tears as a result of repetitive use injuries. This approach can also be used to help prevent an Achilles tendon rupture. If your Achilles tendon has already ruptured or torn, Achilles tendon surgery can be used to reattach the ends of the torn tendon. This approach is more thorough and definitive compared to non surgical treatment options discussed above. Surgical reattachment of the tendon also minimizes the change of re-rupturing the Achilles tendon.
Prevention
Appropriately warm up and stretch before practice or competition. Allow time for adequate rest and recovery between practices and competition. Maintain appropriate conditioning, Ankle and leg flexibility, Muscle strength and endurance, Cardiovascular fitness. Use proper technique. To help prevent recurrence, taping, protective strapping, or an adhesive bandage may be recommended for several weeks after healing is complete.
What Are Primary Causes And Warning Signs Of Achilles Tendon Rupture
Overview

A tendon is a band of tissue that connects a muscle to a bone. The Achilles tendon runs down the back of the lower leg and connects the calf muscle to the heel bone. Also called the ?heel cord,? the Achilles tendon facilitates walking by helping to raise the heel off the ground. The Achilles tendon is at the back of the heel. It can be ruptured by sudden force on the foot or ankle. If your Achilles tendon is ruptured you will be unable to stand on tiptoe, and will have a flat-footed walk. It is important to diagnose and treat this injury as soon as possible, to help promote healing. Treatment involves wearing a plaster cast or brace (orthosis) for several weeks, and possibly having an operation.
Causes
Often an Achilles rupture can occur spontaneously without any prodromal symptoms. Unfortunately the first "pop" or "snap" that you experience is your Achilles tendon rupture. Achilles tendon rupture most commonly occurs in the middle-aged male athlete (the weekend warrior who is engaging in a pickup game of basketball, for example). Injury often occurs during recreational sports that require bursts of jumping, pivoting, and running. Most often these are tennis, racquetball, squash, basketball, soccer, softball and badminton. Achilles rupture can happen in the following situations. You make a forceful push-off with your foot while your knee is straightened by the powerful thigh muscles. One example might be starting a foot race or jumping. You suddenly trip or stumble, and your foot is thrust in front to break a fall, forcefully over stretching the tendon. You fall from a significant height. It does appear that previous history of Achilles tendonitis results in a degenerative tendon, which can grow weak and thin with age and lack of use. Then it becomes prone to injury or rupture. Certain illnesses (such as arthritis and diabetes) and medications (such as corticosteroids and some antibiotics) can also increase the risk of rupture.
Symptoms
Symptoms usually come on gradually. Depending on the severity of the injury, they can include Achilles pain, which increases with specific activity, with local tenderness to touch. A sensation that the tendon is grating or cracking when moved. Swelling, heat or redness around the area. The affected tendon area may appear thicker in comparison to the unaffected side. There may be weakness when trying to push up on to the toes. The tendon can feel very stiff first thing in the morning (care should be taken when getting out of bed and when making the first few steps around the house). A distinct gap in the line of the tendon (partial tear).
Diagnosis
To diagnose an Achilles tendon injury, your health care provider will give you a thorough physical exam. He or she may want to see you walk or run to look for problems that might have contributed to your Achilles tendon injury.
Non Surgical Treatment
Once the Achilles tendon is partially damaged, one should exercise great care. The risk of rupture is high and if pain is associated with walking, one should consult with an orthopedic surgeon or a sports physician. A complete rupture of the Achilles tendon is never treated at home. It is important to understand that there are no minerals, nutrients, or herbs to treat Achilles tendon injury and any delay just worsens the recovery.
Surgical Treatment
The goal of surgery is to realign the two ends of the ruptured tendon to allow healing. There are multiple techniques to accomplish this goal that will vary from surgeon to surgeon. Recovery from this injury is usually very successful with return to full function in approximately 6 months. Post operatively casting is required with the use of crutches or other means to remain non-weightbearing for 4-8 weeks. This is followed by a course of physical therapy. Partial rupture may or may not require surgical intervention depending on the extent of injury but cast immobilization is a common requirement.
Achilles Tendon Rupture How Do I Know I Suffered It?
Overview

Your Achilles tendon is a large band of tissue in the back of your ankle. It connects your calf muscles to your heel bone. The tendon helps you point your foot downward, rise on your toes, and push off when you walk. You use it almost every time you move. But repeated stress can make the tendon more prone to injury. It may become inflamed and develop small tears (tendonitis). A complete tear through the tendon is known as an Achilles tendon rupture.
Causes
Achilles tendon ruptures are most likely to occur in sports requiring sudden stretching, such as sprinting and racquet sports. Achilles tendon ruptures can happen to anyone, but are most likely to occur to middle age athletes who have not been training or who have been doing relatively little training. Common sporting activities related to Achilles tendon rupture include, badminton, tennis, squash. Less common sporting activities that can lead to Achilles tendon rupture include: TKD, soccer etc. Occasionally the sufferer may have a history of having had pain in the Achilles tendon in the past and was treated with steroid injection to around the tendon by a doctor. This can lead to weakening of the tendon predisposing it to complete rupture. Certain antibiotics taken by mouth or by intravenous route can weaken the Achilles tendon predisposing it to rupture. An example would be the quinolone group of antibiotics. An common example is Ciprofloxacin (or Ciprobay).
Symptoms
Tendon strain or tendon inflammation (tendonitis) can occur from tendon injury or overuse and can lead to a rupture. Call your doctor if you have signs of minor tendon problems. Minor tenderness and possible swelling increases with activity. There is usually no specific event causing sudden pain and no obvious gap in the tendon. You can still walk or stand on your toes. Acute calf pain and swelling can indicate a tear or partial tear of the Achilles tendon where it meets the calf muscle. You may still be able to use that foot to walk, but you will need to see a specialist such as an orthopedic surgeon. Surgery is not usually done for partial tears. Sometimes special heel pads or orthotics in your shoes may help. Follow up with your doctor to check for tendonitis or strain before resuming activity, because both can increase the risk of tendon rupture. Any acute injury causing pain, swelling, and difficulty with weight-bearing activities such as standing and walking may indicate you have a tear in your Achilles tendon. Seek prompt medical attention from your doctor or emergency department. Do not delay! Early treatment results in better outcome. If you have any question or uncertainty, get it checked.
Diagnosis
Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis.
Non Surgical Treatment
Achilles tendon ruptures can be treated non-operatively or operatively. Both of these treatment approaches have advantages and disadvantages. In general, younger patients with no medical problems may tend to do better with operative treatment, whereas patients with significant medical problems or older age may be best served with non-operative treatment. However, the decision of how the Achilles tendon rupture is treated should be based on each individual patient after the advantages and disadvantages of both treatment options are reviewed. It is important to realize that while Achilles tendon ruptures can be treated either non-operatively or operatively, they must be treated. A neglected Achilles tendon rupture (i.e. one where the tendon ends are not kept opposed) will lead to marked problems of the leg in walking, which may eventually lead to other limb and joint problems. Furthermore, late reconstruction of non-treated Achilles tendon rupture is significantly more complex than timely treatment.

Surgical Treatment
Surgery may be indicated directly following injury rather than conservative care. Repair of an achilles tendon rupture is greatly varied for each clinical situation. There may be a direct repair of the ends of the tendon with suture, or possibly a tendon graft used to augment the tendon. Post-operatively, the period of immobilization will depend on the size of the defect that was repaired and how it was completed. Usually the immobilization is between 6-10 weeks. This repair may allow for a complete return to normal function, but in many instances the healing is complicated with adhesions and a partial loss of range of motion. There may be a continued soft tissue defect noted and a permanent or prolonged swelling.
About
Fashion is in my blood. When I was a kid, my mom would drive me two hours through crazy LA traffic for photo shoots. I used to hang out with the stylists, try on clothes, get advice. It was a great way to grow up. Eventually, I started giving my friends fashion advice, and never looked back.
After 20 years as a stylist for photographers, I was ready to start a business that would let me evolve my own fashion and consulting style. More than anything, I wanted to share my passion for fashion, and watch as my clients discovered the transformative power of a knock-out look.
Today my clients are CEOs, celebrities, corporate and creative people -- men and women who want serious input on their clothing style, advice on what to wear to an event, or how to put together and pack the most versatile travel wardrobe. I also do styling for fashion shoots, including art direction, makeup, hair, clothing and accessorizing. I’ll make you look great. I promise.